In the first part of this post I re-examined some misleadingly presented data from the US CDC, and then spent a good bit of energy exploring why my immediate instinct was to mistrust the CDC’s reporting. Basically, my “Bayesian priors” about the CDC’s trustworthiness are low, because it’s a government agency and the government lies continually about anything that has a political impact — which is to say in the Age of Wokeness, everything. But this isn’t an acceptable end point — because the data in question is actually pretty important, and we need to be able to arrive at some kind of confidence about our interpretation of it. Does the vaccine work or not? If you are a vaccinated person in a vulnerable group, should you be worried, or should you feel confident going about your life like normal? We can’t stop the CDC from being an unreliable reporter; and we can’t expect any non-state organization to be able to provide this kind of aggregate epidemiological data in a real-time manner; so how can we recognize good science through the noise of political bullshittery? Sometimes (at least theoretically) the CDC publishes data that is both true and not misleading — I know some of these guys and can vouch for their not being completely dishonest or incompetent — so how can we spot the real science in the sea of garbage?
One way to approach this problem is to compare reports from different agencies that are not (at least directly) connected to each other. This of course was where my skepticism about the particular dataset mentioned in my last post started – by comparing it to data from the UK and Israel. One reason I have tended to trust the UK data is that they have been posted consistently on a week-by-week basis since the beginning of the “pandemic”. Because of this, the effect of a sudden politically-driven course correction is much more likely to be visible, reducing the chance that the agencies might think they could get away with fudging or burying inconvenient numbers. But you perhaps can’t use the UK data as a direct comparison with US data, because one could claim that the populations are sufficiently different that you can’t assume the two should look the same. Perhaps, though, we can find some subset of the US data that is trustworthy in the same way that the UK data is, which would make for a good sanity check of the CDC’s numbers.
Some friends and I have followed the COVID reports from Vermont fairly closely since last fall, because they were one of the only states to report reasonably transparent data about “breakthrough” infections. They did this long before you could similar data for the whole country from the CDC, for instance. Because of this reporting schedule, and because Vermont is relatively small and relatively well-off, it avoids some of the potential problems we noted with the US data as a whole. For example, there aren’t many illegal aliens in Vermont — at 0.1% of the total population, it’s in fact the lowest illegal population of all 50 states. Similarly, only North Dakota and Wyoming have lower per capita homelessness rates than Vermont. So we can be much more confident that the denominator of the vaxxed/unvaxxed ratio is well-constrained for this dataset. Let’s see how Vermont’s numbers compare to the country as a whole.
Based on this early February report (and my calculations from it), there were about 18,000 infections in unvaccinated Vermonters in January, and 22,000 infections in vaccinated individuals. So right there is data surprising to a lot of normies: the absolute number of infections is greater in the vaxxed population. When you compare these numbers to the overall census Vermont population of 643,503, 80% of which is vaccinated, you get a 4.2% risk of infection for vaxxed, and a 14.1% risk of infection for unvaxxed, or about a 3.3x lower risk for vaxxed. First of all, stop and consider the fact that more than 6% of the population of the state caught COVID in one month, despite the fact that 80% of its people were “fully vaxxed”. Not exactly glowing support for the vaccine. But my calculation of the efficacy of the vaccine in Vermont is actually slightly better than the estimate from the national data posted by CDC. There might be reasons why it would be elevated — Vermont schools, for instance, require unvaxxed people to test after exposure, but not vaxxed, which probably inflates the unvaxxed rate estimate — but regardless, it’s in the same ballpark, so I think we can safely conclude that the CDC’s data on infection risk reduction from vaccination is roughly accurate.
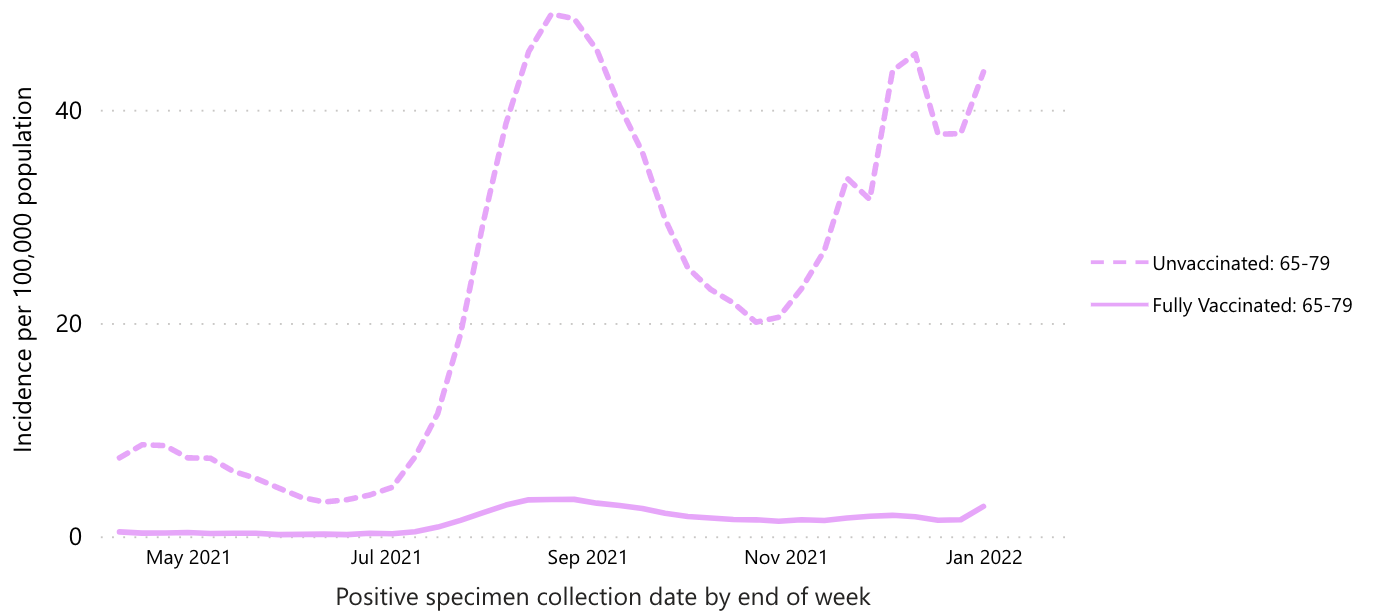
On the other hand, the data on death risk is less convincing. According to the CDC data, the “protection from death” ratio from vaccination is something like 20-30x. The graph below focuses only on the 65-79 year old age group, since that’s the one where the vast majority of COVID-only deaths have occurred:
In Vermont, though, the improvement is roughly the same as the improvement in terms of infection risk. You have to do some crunching to get these numbers as I couldn’t find a place to get the raw numbers, but here’s my thinking. There have been 566 total deaths in Vermont through January 2022, and 65, or 11.5%, of those occurred in January. There have also been 157 deaths in fully vaccinated Vermonters, but I couldn’t find how many of those occurred in January. If we assume that the same overall percentage of them – 11.5% – occurred in January, than that’s 18 vaxxed January deaths, compared to 47 unvaxxed deaths. That’s a ratio of only 2.6, fully an order of magnitude less protection than the CDC (and nearly all other sources, including anti-mandate sources) claims. If we calculate the numbers based on risk of death after infection, 18 of 21,800 vaxxed COVID patients died in January (0.08%), compared to 47 of 18,200 unvaxxed (0.26%), for a factor of 3.1x protection. Again, much less protection than CDC claims. Still probably enough to justify getting vaxxed if you’re miraculously still COVID-naïve and don’t believe the vaxx causes heart attacks, but way less than the regime’s vaxx propaganda claims. I will note that this was exactly what my friends and I observed in the Vermont data back last fall – a much much lower estimate of protection vs. death in Vermont than in the nationwide data.
So who should you trust? We’re back to our Bayesian priors again, aren’t we? My feel is that you should immediately trust the smaller organization more than the larger, because data falsification or bad-actor behavior would be more visible in the small Vermont health care community than in the whole of the US. Vermont is also a very civilized place that is likely to keep fine records and have relatively high amounts of scruples about accuracy, honesty, and so forth, at least compared to the weasels in DC.
But the real reason I trust the Vermont numbers is that they suit my scientific priors, not just my political ones. Briefly, it just doesn’t make any sense for the vaccine to provide superior protection against death than against infection in general. If the vaccine-induced antibodies are capable of identifying and killing COVID-infected cells sufficiently to reduce serious outcomes, why wouldn’t they also be able to do it to mild infections? One would expect them to provide similar reductions in risk for all outcomes of viral infection, not dramatically higher protection against death than sniffles. In Vermont, the vaccine provides similar levels of protection against both infection (i.e. testing positive for COVID) and death, which makes a lot more sense than the completely bizarre observation of 10x greater protection from death than from infection.
For these reasons I’m strongly leaning toward trusting Vermont and accusing CDC of lying. In the absence of a coherent scientific explanation, the best explanation for why vaccine-induced antibodies would protect against death but not sniffles is that voters care about death a lot more than they care about sniffles. Plus it’s a hell of a lot easier to conceal the true death rate than the sniffle rate. Most of us don’t know anybody who has died of COVID, but for the last month we’ve watched tons of people (mostly fully vaccinated) catch it. So CDC presents an honest picture of vax protection against infection, but fudges things somehow (I am not sure how) to reduce the death rate in the vaccinated. But we’ve all seen how the death rate can be manipulated up or down based on what we count as a COVID death — so it’s very easy to imagine this number can be gamed by the aggregators at CDC on command of their political bosses.
The tragedy of all of this is that I even have to ask these sorts of questions. We truly live in an informational void, where you can’t readily trust anything that you don’t see with your own eyes. And the frequency with which some media outlet tells you that what you personally saw happen never happened is disturbingly high. What are the long-term consequences of this disintegration of credibility in our institutions? What does the world look like when you can’t trust your doctors anymore? It’s like some kind of singularity – we are sitting on the event horizon of a world that people born in the United States can barely imagine.
One great thing about taking a Bayesian approach to issues like this is that it gives us a way to understand people we disagree with — you have to address their priors, which may be different from yours for good reason. If their priors are different, and are not completely unreasonable, then it’s fairly easy to “agree to disagree”. It also might tend to steer contentious conversations toward those priors, instead of the proximal issue of disagreement, which might lead to deeper understanding and compassion, and help us as a society step back from the precipice upon which we are teetering. If enough of my scientific colleagues could embrace this worldview and performatively model it for the public, I truly believe it would make a difference. Alas, my priors are strong that this will not happen — but I would love to be proven wrong.


One wonders why, with no explanation of the science, the FDA early on approving the use of HCQ only be used in hospitals–no approval for outpatient use, where an antiviral might actually help.
Also, one wonders why the CDC, in Jan. 2020, recommended that high risk influenza patients be treated early, even before receiving test results–on the basis of clinical suspicion–with antivirals. Yet there was no recommendation or advisory to treat covid with HCQ for the same cohort.
Have the FDA and CDC abandoned their regulatory role to become partners with pharma?