A very interesting analysis came out today of Pfizer’s decision to forego announcing the success of their COVID-19 vaccine clinical trials until a few days after the 2020 US presidential election was over. In case you have forgotten, in 2020 President Donald Trump initiated a Manhattan Project scale effort — “Project Warp Speed” — to develop and release a vaccine against the virus that was infecting everyone’s brainsamygdalas respiratory tracts. I didn’t believe the effort would succeed, since the fastest I was aware of any vaccine ever being approved for release was about five years; in retrospect I still don’t think the trials succeeded, although this wasn’t really Pfizer’s fault, as if the vaccines had been deployed sensibly instead of being forced universally on the world’s population they might still work today, and that was a government decision, not a corporate one. But the question of whether or not the vaxx was “safe and effective” is not the subject of this post — the question is, why did Pfizer wait to reveal the results of their trial until it had no chance of helping Donald Trump’s electoral desirability? To quote the article:
In the alternate universe where the 32-case interim analysis was conducted as set forth in the original study protocol, The New York Times would have run a full page headline declaring the success of the Pfizer Covid-19 vaccine right around the morning of November 2nd, the day before the election… On a political level, you’ll have to confer with Nate Silver on whether the Pfizer news would have been enough to swing 100,000 votes in Pennsylvania, 30,000 votes in Wisconsin, and 20,000 votes in Georgia and put Donald Trump back in the White House… What’s truly crazy is that a few pharma executives, unaccountable to both the public and their shareholders, got to make this crucial decision, and that they got away with it without a hint of a congressional subpoena.
Like so many other things about the 2020 election, this smacks of conspiracy, committed by the deracinated, unelected, and mostly incompetent oligarchical elites of the United States to hamstring the grassroots nationalist insurgency represented by the Trump regime and that threatened their status. If one believes that the vaxx is “safe and effective” then it must be acknowledged that the choice made by Pfizer delayed the full-scale deployment of the vaccine for a couple of weeks, and in the winter of 2020-2021 that represented literally tens of thousands of human lives lost. But regardless of its ultimate efficacy, millions of Americans were eagerly awaiting some good news about their lives returning to normal, and their opinion of Trump’s handling of the “pandemic” — which was deeply underwater just before the election — likely would have changed dramatically. Executives at Pfizer, in all likelihood in collusion with government officials at NIH such as Francis Collins and Anthony Fauci, made a conscious decision to manipulate the election by withholding the results of mission critical federally-funded research from the public. At a minimum this is the grossest kind of violation of professional ethics for a scientist; but I believe it is also a clear-cut violation of several federal laws such as the Hatch Act that prevent the involvement of agencies like NIH with the political process in the US. A serious country would investigate it; but of course our investigatory agencies like the FBI are clearly “in on it”, judging by the revelation of their election-rigging activities at Twitter.
In a post I released immediately before the 2022 midterm elections, I argued that the only way the US returns to normal is either through something akin to a civil war, or a collective mea culpa or other type of debt-paying by the elites that have brought us to this dire juncture in our history. One form that mea culpa could take is something like a Nuremberg trial for the people responsible for the “pandemic” and all of its metastatic outgrowths, including the rigging of the 2020 US Presidential election. It’s possible that the current crop of congress-critters might at least bring them to question, but I highly doubt anything of consequence will happen to them — or at least not many of them; they may throw someone to the wolves but it will just be for theatrical purposes. The oligarchy protects its own.
In case you’re paywalled, it’s an argument that we need to significantly alter the way we teach introductory college science courses, because obviously the common people of the West can’t reason scientifically.
OK, sure, on some level I agree with the sentiment. I’ve been a vocal advocate for higher education reforms for quite some time now, and I teach my own classes using the kinds of “active learning” reforms advocated by the article’s authors. Broadly speaking, there’s a conflict amongst college instructors on whether it’s more important to “cover all the content” in a class, or instead focus on deeper engagement with core competencies and practical skills. The former argue that there is a massive knowledge base necessary for somebody to understand modern biology, which is true – and therefore that we have to cover all of it in our two-semester introductory biology sequence. The latter (including me) argue that it’s pointless to have a professor stand at the front of a class and recite the litany of biology sensu lato if the end result is basically students “drinking from a fire hose” and retaining less than 10% of the content, which is what survey after survey shows is what they actually get out of intro bio. The authors of this article, and I, believe it is more effective to choose a good 10% of “content” and cover it in greater detail, making sure to relate it back to the core themes of the discipline so that students build a strong base that they can expand on later as they take more specialized higher-level courses.
Ok, but whatever, nobody reads ASD to get my hot takes on university pedagogy. What struck me about this article was how they started it. Here’s the first paragraph:
The rapid development of highly effective vaccines against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was a monumental achievement, yet a large fraction of the public rejected this means of defense, resulting in far too many preventable deaths. This response reflects a shocking failure of science to produce citizens who understand and respect scientific evidence, and it demands a rethinking of science education goals.
First it strikes me as wild that you would lead off an article about scientific illiteracy with a highly dubious claim – that lack of vaccination in some portion of the public resulted in increased deaths – without any citation to a published study, relying simply on what we were all supposed to imbibe from the CDC’s press releases about the effect of vaccination on COVID outcomes. I’ve expressed my skepticism of this claim – based on data – before.
But that’s not even the worst bit. To me, what really stands out about this paragraph is its utter lack of engagement with the arguments made by that “large fraction of the public”. I suspect that the large majority of you who are reading this sympathetically (as opposed to the commie trolls that stumble in here from time to time) came to your mistrust of the COVID vaccines because of scientific reasoning, not because of some half-baked conspiracy theory or a lack of “respect” for science. If you were like me, alarm bells started flashing like crazy when the CDC maintained that even people who had recovered from COVID infections could garner some benefit from the vaccine. That claim was utterly baseless – the CDC “study” supporting it was laughably bad – but to a first approximation everybody in professional science took it as gospel. There was also the evidence that the vaccine failed to stop infection and transmission, that I’ve written about before, which made it obvious that the vaccine would fail in short order. And of course eugyppius documented so many more of your reasons for mistrusting the party line on vaccines, all of them reasonable, all of them based on data and observation – in short, reflecting the best kind of citizen science we could possibly hope to see.
So far from reflecting a failure of scientific education, it seems to me that the mass rejection of the baseless claims of the vaccinators reflects a remarkable success of scientific education. Our leaders attempted to hoodwink us with garbage statistics and opaque data sources to get us to take a drug they had to already know would not provide any kind of long term benefit, but we caught them because we can think scientifically. We obviously aren’t as stupid or as gullible as they thought, and we obviously learned a thing or two from our science teachers about scientific reasoning.
But perhaps that opening paragraph has a nugget of sensibility in it after all – consider this phrase (emphasis mine):
a shocking failure of science to produce citizens who understand and respect scientific evidence
It seems to me that science education can get people to either understand or respect scientific evidence, but not both. What does it mean to “respect” scientific evidence? Probably what the authors intend is the idea that one should be willing to change their view about something based on solid scientific evidence. But based on what we know about the reality of the vaccine, one has to conclude that their idea of “respect” for science means “respect for scientists”, or better yet “submission to scientists’ opinions”. Far from wanting the public to be more capable of scientific reasoning, they want them to be less capable, and more dependent on the received wisdom from the academic Cathedral rather than their own reasoned opinion. Were it otherwise, our scientific vicars would have acknowledged our criticisms of their data and attempted in good faith to refute them, rather than doubling down with propaganda and government force and coercion. The fact that, at this late date, you can get an article like this published in Science without acknowledging that vaccine critics made at least a few concerning points, is prima facie evidence that capital-s Science has no concern whatsoever for the general public’s ability to think scientifically for itself.
Ironically, like many professional scientists, the authors of this article appear to live in an isolated world where they don’t have to actually think about much. Basically, everybody you see every day either agrees with you about basically everything of consequence, or else is too afraid of being cancelled to contradict you. Scientists like this are so cloistered that they can just tell themselves, with no evidence, that vaccine rejection is caused by lunatic conspiracy theories about lizard people or white genocide or whatever, and the public are just rubes who will fall for anything. Their “blaming” of science education is sort of a humble-brag – it highlights their superiority over you plebe losers, who can’t grasp scientific arguments because you haven’t been fully blessed with their gnosis. If you want a better explanation for the utter failure of our response to the coronavirus, look to the insularity, uninquisitiveness, and authoritarianism of academic science, who, having pushed as many dissenting voices into the outer darkness as possible, have lost the capacity to effectively “peer review” their own attitudes.
In the first part of this post I re-examined some misleadingly presented data from the US CDC, and then spent a good bit of energy exploring why my immediate instinct was to mistrust the CDC’s reporting. Basically, my “Bayesian priors” about the CDC’s trustworthiness are low, because it’s a government agency and the government lies continually about anything that has a political impact — which is to say in the Age of Wokeness, everything. But this isn’t an acceptable end point — because the data in question is actually pretty important, and we need to be able to arrive at some kind of confidence about our interpretation of it. Does the vaccine work or not? If you are a vaccinated person in a vulnerable group, should you be worried, or should you feel confident going about your life like normal? We can’t stop the CDC from being an unreliable reporter; and we can’t expect any non-state organization to be able to provide this kind of aggregate epidemiological data in a real-time manner; so how can we recognize good science through the noise of political bullshittery? Sometimes (at least theoretically) the CDC publishes data that is both true and not misleading — I know some of these guys and can vouch for their not being completely dishonest or incompetent — so how can we spot the real science in the sea of garbage?
One way to approach this problem is to compare reports from different agencies that are not (at least directly) connected to each other. This of course was where my skepticism about the particular dataset mentioned in my last post started – by comparing it to data from the UK and Israel. One reason I have tended to trust the UK data is that they have been posted consistently on a week-by-week basis since the beginning of the “pandemic”. Because of this, the effect of a sudden politically-driven course correction is much more likely to be visible, reducing the chance that the agencies might think they could get away with fudging or burying inconvenient numbers. But you perhaps can’t use the UK data as a direct comparison with US data, because one could claim that the populations are sufficiently different that you can’t assume the two should look the same. Perhaps, though, we can find some subset of the US data that is trustworthy in the same way that the UK data is, which would make for a good sanity check of the CDC’s numbers.
Some friends and I have followed the COVID reports from Vermont fairly closely since last fall, because they were one of the only states to report reasonably transparent data about “breakthrough” infections. They did this long before you could similar data for the whole country from the CDC, for instance. Because of this reporting schedule, and because Vermont is relatively small and relatively well-off, it avoids some of the potential problems we noted with the US data as a whole. For example, there aren’t many illegal aliens in Vermont — at 0.1% of the total population, it’s in fact the lowest illegal population of all 50 states. Similarly, only North Dakota and Wyoming have lower per capita homelessness rates than Vermont. So we can be much more confident that the denominator of the vaxxed/unvaxxed ratio is well-constrained for this dataset. Let’s see how Vermont’s numbers compare to the country as a whole.
Based on this early February report (and my calculations from it), there were about 18,000 infections in unvaccinated Vermonters in January, and 22,000 infections in vaccinated individuals. So right there is data surprising to a lot of normies: the absolute number of infections is greater in the vaxxed population. When you compare these numbers to the overall census Vermont population of 643,503, 80% of which is vaccinated, you get a 4.2% risk of infection for vaxxed, and a 14.1% risk of infection for unvaxxed, or about a 3.3x lower risk for vaxxed. First of all, stop and consider the fact that more than 6% of the population of the state caught COVID in one month, despite the fact that 80% of its people were “fully vaxxed”. Not exactly glowing support for the vaccine. But my calculation of the efficacy of the vaccine in Vermont is actually slightly better than the estimate from the national data posted by CDC. There might be reasons why it would be elevated — Vermont schools, for instance, require unvaxxed people to test after exposure, but not vaxxed, which probably inflates the unvaxxed rate estimate — but regardless, it’s in the same ballpark, so I think we can safely conclude that the CDC’s data on infection risk reduction from vaccination is roughly accurate.
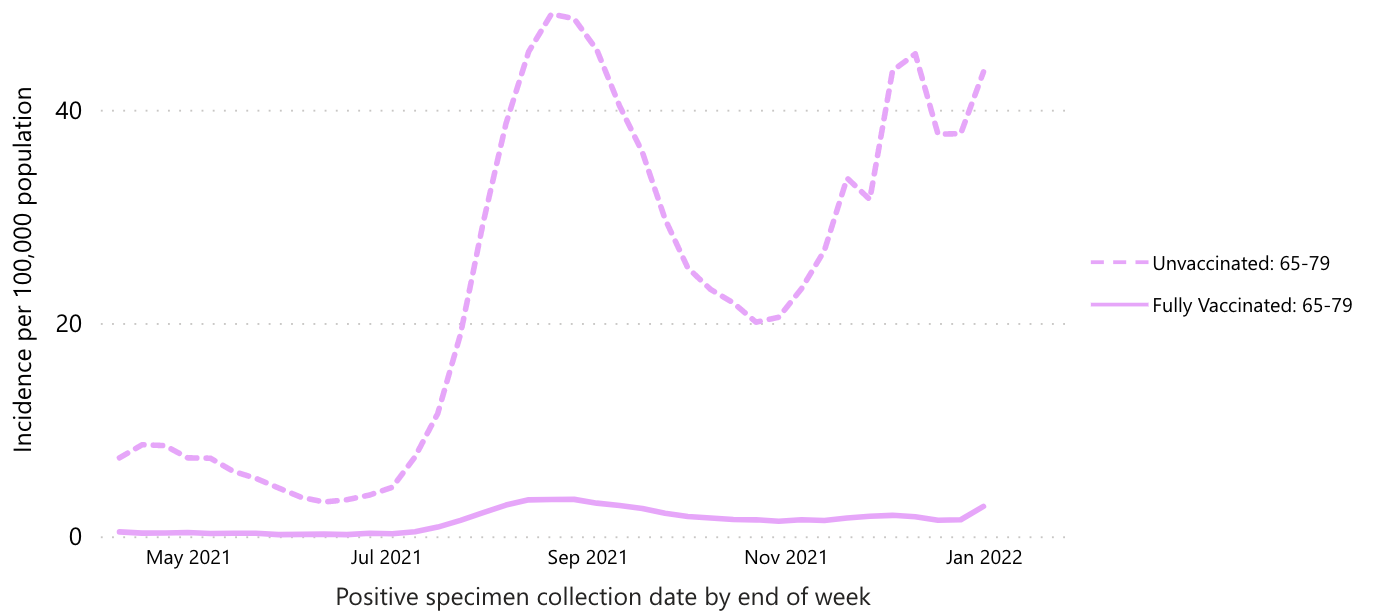
On the other hand, the data on death risk is less convincing. According to the CDC data, the “protection from death” ratio from vaccination is something like 20-30x. The graph below focuses only on the 65-79 year old age group, since that’s the one where the vast majority of COVID-only deaths have occurred:
In Vermont, though, the improvement is roughly the same as the improvement in terms of infection risk. You have to do some crunching to get these numbers as I couldn’t find a place to get the raw numbers, but here’s my thinking. There have been 566 total deaths in Vermont through January 2022, and 65, or 11.5%, of those occurred in January. There have also been 157 deaths in fully vaccinated Vermonters, but I couldn’t find how many of those occurred in January. If we assume that the same overall percentage of them – 11.5% – occurred in January, than that’s 18 vaxxed January deaths, compared to 47 unvaxxed deaths. That’s a ratio of only 2.6, fully an order of magnitude less protection than the CDC (and nearly all other sources, including anti-mandate sources) claims. If we calculate the numbers based on risk of death after infection, 18 of 21,800 vaxxed COVID patients died in January (0.08%), compared to 47 of 18,200 unvaxxed (0.26%), for a factor of 3.1x protection. Again, much less protection than CDC claims. Still probably enough to justify getting vaxxed if you’re miraculously still COVID-naïve and don’t believe the vaxx causes heart attacks, but way less than the regime’s vaxx propaganda claims. I will note that this was exactly what my friends and I observed in the Vermont data back last fall – a much much lower estimate of protection vs. death in Vermont than in the nationwide data.
So who should you trust? We’re back to our Bayesian priors again, aren’t we? My feel is that you should immediately trust the smaller organization more than the larger, because data falsification or bad-actor behavior would be more visible in the small Vermont health care community than in the whole of the US. Vermont is also a very civilized place that is likely to keep fine records and have relatively high amounts of scruples about accuracy, honesty, and so forth, at least compared to the weasels in DC.
But the real reason I trust the Vermont numbers is that they suit my scientific priors, not just my political ones. Briefly, it just doesn’t make any sense for the vaccine to provide superior protection against death than against infection in general. If the vaccine-induced antibodies are capable of identifying and killing COVID-infected cells sufficiently to reduce serious outcomes, why wouldn’t they also be able to do it to mild infections? One would expect them to provide similar reductions in risk for all outcomes of viral infection, not dramatically higher protection against death than sniffles. In Vermont, the vaccine provides similar levels of protection against both infection (i.e. testing positive for COVID) and death, which makes a lot more sense than the completely bizarre observation of 10x greater protection from death than from infection.
For these reasons I’m strongly leaning toward trusting Vermont and accusing CDC of lying. In the absence of a coherent scientific explanation, the best explanation for why vaccine-induced antibodies would protect against death but not sniffles is that voters care about death a lot more than they care about sniffles. Plus it’s a hell of a lot easier to conceal the true death rate than the sniffle rate. Most of us don’t know anybody who has died of COVID, but for the last month we’ve watched tons of people (mostly fully vaccinated) catch it. So CDC presents an honest picture of vax protection against infection, but fudges things somehow (I am not sure how) to reduce the death rate in the vaccinated. But we’ve all seen how the death rate can be manipulated up or down based on what we count as a COVID death — so it’s very easy to imagine this number can be gamed by the aggregators at CDC on command of their political bosses.
The tragedy of all of this is that I even have to ask these sorts of questions. We truly live in an informational void, where you can’t readily trust anything that you don’t see with your own eyes. And the frequency with which some media outlet tells you that what you personally saw happen never happened is disturbingly high. What are the long-term consequences of this disintegration of credibility in our institutions? What does the world look like when you can’t trust your doctors anymore? It’s like some kind of singularity – we are sitting on the event horizon of a world that people born in the United States can barely imagine.
One great thing about taking a Bayesian approach to issues like this is that it gives us a way to understand people we disagree with — you have to address their priors, which may be different from yours for good reason. If their priors are different, and are not completely unreasonable, then it’s fairly easy to “agree to disagree”. It also might tend to steer contentious conversations toward those priors, instead of the proximal issue of disagreement, which might lead to deeper understanding and compassion, and help us as a society step back from the precipice upon which we are teetering. If enough of my scientific colleagues could embrace this worldview and performatively model it for the public, I truly believe it would make a difference. Alas, my priors are strong that this will not happen — but I would love to be proven wrong.
A few days ago Steve Sailer posted some recent graphs of US COVID cases (and deaths) in unvaxxed vs. vaxxed vs. boosted individuals that I found first surprising, then completely implausible. The graphs come from this CDC website – I’m not sure how long it has been up, but the “publications” cited in the fine-print footnotes are, at the earliest, from September last, and this is the first time I’m seeing some of these numbers, so I’m guessing it is a reasonably recent tool. Regardless, here’s the graph that Steve posted:
Which certainly gives the impression that the vaccine (and its booster) not only provides powerful protection against infection, but that the degree of protection has remained consistent for months. I found this completely unbelievable, because if nothing else the steady rate of infection of the unvaxxed should cause them to become less and less susceptible over time — a recovered individual is at least as resistant as a vaxxed one — so it’s prima facie implausible that the level of relative protection wouldn’t decrease. For comparison, here is a graph from the same website that shows broader context, including the period prior to “boosting”:
Which shows a bit more fluctuation in vaccine efficacy, but still lends the impression that it remains highly effective. But my bullshit detector goes off whenever I see anything from the CDC at this point, so I decided to look a little closer — it’s easy to mislead with graphs. While I wasn’t able to download the raw data directly (not willing to go plowing through subpages to find a link), I was able to extract enough info from the graphic charts to make this rough plot which I think is more informative:
Clearly the efficacy of the vaccines is waning over time. The suddenness of the shifts – from roughly 10x protection in this data set, down to 4-5x, down to 2x and dropping, is consistent not with the waning of vax-induced antibodies, but (as I have argued before on this blog) with the documented selective sweeps of vaccine-resistant viral genotypes Delta and Omicron occurring in summer and winter 2021 respectively. In other words, it is unreasonable to think a booster shot of the same vaccine could provide any benefit – at least not an immunological benefit, although it’s possible I suppose that inducing a chronic state of inflammation or high-level immune preparedness could reduce symptoms somehow, probably with a trade-off in terms of increased risks on other fronts, like heart disease (short term, and already observed, at least anecdotally, by many of us) and cancer (longer term, especially for anyone foolish enough to keep this jab insanity going for years). Based on the trend in the graph, I would anticipate that the next variant would render the vaccine completely obsolete, even based on this CDC data.
Something similar is observed with the CDC’s data on death rates. Here’s their graph (again, from Steve’s blog):
And here is my re-creation, showing ratios of unvaxxed:vaxxed rates (focusing only on the 65-79 age group, since it is the only age group likely to represent actual COVID deaths in great enough numbers to be meaningful):
So not much evidence of the same trend. In fact, no real trend at all, other than that the vaccine provides strong protection against the worst outcomes. Hmm.
I don’t intend this to be just a “analyze the vaxx data” post. What I’m interested in, is why my first thought when I saw the data was to be suspicious of it. Am I paranoid? Have I gone full anti-vaxxer, to the point that I instantly start looking for reasons to refute pro-vax information? I don’t feel anti-vaccine; I would still encourage people to get tetanus shots, for instance, and am tentatively still supportive of childhood vaccination (although I have learned there is a lot about that practice that I have taken for granted which is apparently not entirely true). I’m certainly not “anti-science”, as is hopefully obvious based on my career choice. Maybe, then, there’s something else afoot that prompts me to sneer at the CDC’s graphs and probe their data when most of my colleagues just shrug their shoulders and move on? Let’s look closer and find out.
What we are dealing with here is an issue of Bayesian inference. In simple terms (and I don’t want to suggest I could explain it in more complicated ones), Bayes’ theorem describes the conditions which should cause a reasonable person to change their mind about something. Briefly, the more confident you are of a pre-existing (or prior) belief, and the less confident you are in the trustworthiness of a new piece of evidence, the more hesitant you should be to update your original belief. When you hear somebody say something about “updating their priors”, that’s what they’re talking about. It’s also how two people can look at the same exact evidence, and one of them be convinced while the other remains skeptical — it’s about the strength of their priors and their evaluation of the evidence’s plausibility.
Suffice it to say, my priors after two years of pandemic porn are “The CDC manipulates data to fool people into doing what the regime wants them to do” and “The CDC are politicians, not scientists” and “Politicians don’t give a single shit about the truth”. So a graph, on its own, is highly unlikely to change my mind in my conviction that the COVID vaccines are garbage. But let’s dissect all those priors, and how they pertain to this particular dataset, to see if I am being unfairly picky.
What initially surprised me about the graphs Steve posted was that the CDC data showed any effect of the vaccine at this point, because the UK and Israeli data have been pretty unequivocal in their conclusion that “double-vaxxed” is “unvaxxed”, i.e., the vaccine provides no protection — at best. The CDC webpage is pretty short on methods, but they do claim that the data are unadjusted, just like the UK data which show unvaxxed having half the rate (or less) of testing positive as vaxxed. The data appear to be collected directly from state health departments in about half of the states in the US, so it’s probably a fairly representative sample. My priors tell me that it’s unlikely that the US numbers are any different than the UK’s and Israel’s; but our political situation is quite different, so it’s highly likely that the CDC is fudging something to make their numbers look better. Is this plausible?
I can imagine three problems that could lead to the differences between the US rate estimates and the UK/Israeli data. All three are easily foreseeable by careful scientists; two of them are understandable but should at least be acknowledged in the report, but the third ought to be grounds for being drawn and quartered. So let’s look at them. First, there could be differences in testing regimes in the three countries. Ever since the beginning of the pandemic it’s been clear that randomized testing of the entire population reveals many cases that would be invisible if we only tested people with symptoms. In many parts of the US, people without vax papers are required to test regularly to participate in normal life. Therefore, it is much more likely that mild infections will be detected in the unvaxxed than the vaxxed, artificially inflating the numerator of the rate estimate (thus making it go up). This is probably less of an issue in the UK and Israel, where the unvaxxed have just been excluded, period, from everything for several months, so no need to test them any more than anyone else*.
Second, it’s possible that there is a problem with the denominator of the rate estimate – the relative population sizes of vaxxed vs. unvaxxed. According to the CDC site, in order to be considered vaccinated, a person had to have a record in their name of receiving both vaccine doses, and the size of the total population was estimated from the US Census data. Both of these could be grievously wrong because of the massive size of the “undocumented” population in the US. By some estimate there could be 30 million illegal aliens inside the US borders right now – roughly 10% of the total population of the country. There are also massive populations of “homeless” and other distressed individuals whose papers are likely not in very good order. These individuals are almost uniformly poor and urban and therefore vastly more likely to contract any communicable disease, by definition. One, when they get tested, they’ll be marked “unvaxxed” whether they are or not (presumably we’re trying to vaccinate these people with or without ID, right?), because there will be no record of their existence in any database, which would artificially increase the unvaxxed rate (and decrease the vaxxed rate). Two, the total population estimate is likely too low, potentially by quite a lot, which would artificially decrease the unvaxxed rate. So the vaxxed rate is probably a pretty good estimate, but the unvaxxed rate is a total crapshoot. There’s also this weird caveat in the CDC’s fine print (emphasis mine):
A continuity correction has been applied to the denominators by capping the percent population coverage at 95%. To do this, we assumed that at least 5% of each age group would always be unvaccinated in each jurisdiction. Adding this correction ensures that there is always a reasonable denominator for the unvaccinated population that would prevent incidence and death rates from growing unrealistically large due to potential overestimates of vaccination coverage.
This suggests that enough regions are reporting > 100% vaccination rates that the data has to be scaled somehow to fix this unrealistic number. It’s harder to explain how the estimates of vaccine coverage could be wrong than how the unvaccinated number could be messed up – it seems, well, sloppy. Which could be said of a lot of government activity in the US, which should lend a good bit of skepticism to any consideration of these data.
Both of the above methodological caveats are understandable, except for the fact that the people reporting these things are supposed to be epidemiological experts who ought to know how to do this sort of data collection and number crunching in a straightforward and honest way. But a third possibility is that the reporting agencies are just lying. On one level this possibility seems remote because so many entities are involved in the testing and reporting apparatus. On the other hand, you have to remember that the public doesn’t have access to any of that raw data, only the aggregates that are posted online, usually by government agencies like CDC. So if CDC’s policy was to “curate” or otherwise alter the data before releasing it, there would be no way for most people to know – including any of the individual reporting entities, none of whom know much about the numbers being reported by other entities. So it comes down to, how much do you trust these ultimate reporting agencies to be honest? Given the state of things in the West, the reasonable position is, basically not at all; if CDC, a political organization, could benefit the regime by falsifying data, and they thought they could get away with it, they would 100% lie.
So is it reasonable that I find the CDC’s data sketchy, or am I a paranoid anti-vaxxer? Bayes’ theorem tells us that it might very well be the case that the CDC’s numbers are accurate, and nevertheless that one would still be justified in evincing skepticism. If my prior expectation is that an information source is compromised or untrustworthy, then the bar goes up for how iron-clad the data has to look before I trust it. If you trust the US government then i) what the fuck is wrong with you, and ii) you are much more likely to trust the CDC’s reports as presented than I am. If on the other hand you’ve noticed that they lie about all sorts of shit all the time, and that every agency of the government appears to be compromised to some degree by boot-licking wokery, then you are far less likely to believe that any government agency could be expected to conduct objective science without undue political influence and bias. If you acknowledge that it is reasonable to mistrust government data drops, then you acknowledge that my skepticism (and that of the many people who are thinking about this the way I am) deserves to be treated with some respect.
In the next post I’ll probe a little deeper into some of this data and try to find a way to “ground-truth” the data. I’ll also consider some other reasons my priors are weighted against the CDC’s report — scientific reasons, not political ones.
* Update — I overstated the degree to which the unvaxxed have been excluded from UK society, and indeed it looks like they do have a problem of over-testing the unvaxxed. Which would mean that the evidence of vaxx failure shown in the UKHSA data is actually underestimated — creating an even bigger discrepancy between the CDC’s numbers and the UK’s.
This post got too long, so I decided to break it up into two somewhat independent pieces. The second half will be released in a few days.
One of the things that evolutionary biologists do, is to look at competitions from the perspectives of relative pay-offs to competitors for different strategies – i.e., game theory. For some time now I’ve been looking at the American political divide in these terms, using one very simple and straightforward framework. I think this framework started in the US but has spread outwards to much of the world where American media is routinely consumed. I also think it is incredibly destructive, and it is difficult to see how to displace it.
Imagine two political parties. One party is largely seen as the party of the wealthy and successful, or at least of people who are mostly content with their lives as they are and do not want to change them. The other party is the exact opposite – the majority of its constituents are either poor, perceive themselves to be victims of some sort, or both; they are not happy with the status quo and want it to change. I think it is reasonable to perceive the Republican Party as the first party, and the Democrat Party as the second. One could retort that Republicans are quite angry these days, but that doesn’t disrupt the framework, because what Republicans are angry about are the extreme ways that Democrats are trying to change Republicans’ lives against their will. Using the hoary terminology of the legacy left, they are reactionaries, reacting against the agendas of the grievance party.
One might look at the state of the lives of many Democrats in the US and sympathize with their desire to change things; there are, no doubt, many injustices and hardships out there. The problem, though, with the framing of our politics becomes evident when we consider the competition between these two parties, and the victory conditions that obtain. Imagine a district that is 49.9% Republican and 50.1% Democrat. How do the Republicans go about reaching a majority? If we agree with the definition of the two parties above, their goal should be to make 0.2% of the population more content with their lives. To do this, they can either a) drug them, or b) actually improve their lives in some noticeable way. Solution (a) is not easily achieved, therefore one expects that the Republicans in such a district will be motivated to help the people of their district – in other words, to do the sorts of things that most of us believe good politicians should do.
What about in the opposite case, in a 50.1% Republican, 49.9% Democrat district? The answer is clear. To attain an electoral majority, the Democrats should create conditions that hurt their constituents, or at least convince their constituents that they have been hurt – victimized – in order to make them aggrieved enough to leave the Republicans and vote Democrat. Anything a Democrat politician did that actually improved the lot of their constituents would necessarily drive some fraction of them into the arms of the Republicans, eventually returning power to the other side. Therefore, if they want to retain their positions, it is in their interest to tighten the screws and keep the suffering hot.
There’s ample evidence that this is exactly what they do. If we discount the plethora of Democrat policies exclusively geared toward rigging elections (e.g., “election reform” and immigration policies), the biggest disconnects between Republicans and Democrats are on how the government should deal with issues of race, climate, and COVID. In all of these cases, Democrat messaging aggressively hyperbolizes threats, creating a sense of impending doom in voters over problems that are relatively minor, if they exist at all. The agitated citizens are then, in principle, motivated to vote for Democrats to protect them from the imminent existential threats they believe in because of the efforts of Democrat PR teams and ground-level activists. Sure, people sometimes behave erratically when under the influence of terrorizing propaganda, doing things like burning police precincts, attacking government buildings, ambush-murdering police officers, advocating imprisonment of unvaxxed people, or foregoing reproduction to “save the planet”. But none of that matters, because politics is a machine optimized for winning elections; within the framework described above, any strategy that doesn’t increase voter fear and suffering will result in Republican victories, and therefore any candidate that moves toward sanity will be defeated by one who moves farther toward the Chicken Little extreme.
Don’t believe me? Consider the chart below, which shows interest in the term “Black Lives Matter” over time, according to Google Trends. The vertical dashed lines correspond to the presidential elections of 2016 and 2020.
This image should dash to pieces any illusions one might have that BLM is a grassroots movement focused on injustices in the black community. Did police suddenly stop shooting unarmed blacks from 2017-2020? If so, why didn’t BLM give President Trump a medal for this amazing downturn in racist violence? If not, why did BLM – presumably a well-organized coalition of activist groups – apparently evaporate during that time period? The simplest answer is that BLM is a direct agent of the Democrat party, existing to drum up hysteria in the black community – and increasingly in the itinerant university community as well – in the run-up to elections, as a tool to “get out the vote”. The massive sudden spikes in interest correspond to injections of propaganda, executed through Democrat media flunkies, followed by what looks like exponential signal decay, as the chaos is allowed to relax after it has done its job.
But so what? All politicians have to try to get people excited about their campaigns in order to get elected. What’s different about this strategy is that it fucks people up severely. Leaving aside the undeniable fact that the BLM movement rioted all over the country in both 2016 and 2020, what’s even worse is that the propaganda used to start those riots left tens of millions of people with dangerously false beliefs about the world they live in. Statistical analysis does not support the hypothesis that police are more likely to shoot blacks than whites in an encounter. But the BLM propaganda machine reinforces the exact opposite belief. How does it affect the minds of everyday people to go about their daily lives believing that they are surrounded by racists and murderers, and how does it impact how one would deal with a police interaction if one goes into it believing the police are likely to kill them for no reason? It must keep them in a constant state of anxiety and worry, and lead them to mistrust many people they encounter who bear them no ill will – indeed, it may even encourage self-destructive behavior.
COVID hysteria is cut from the same cloth. I don’t think that Democrats literally created COVID to win the 2020 election, but they certainly exaggerated it to great effect. They pushed fear of the virus the same way they pushed fear of cops to get the BLM surge started, with the same intent – to blame it on the President they were trying to defeat. Terrified people shut down their economies, destroying the one great victory of the Trump administration – the best financial situation for most people in at least a generation. They mau-maued research into therapeutics that might have brought a swift reduction in death rates and defused the general public’s fear of the virus. They pushed useless mask mandates that created a constant reminder of how terrifying everything was, and reminded you at every turn it was all Trump’s fault, somehow. And infamously, they used fear of the virus to change election laws in swing states to make it easier to harvest ballots from politically disinterested “citizens”, impossible to tell who voted, or tell if anybody cheated.
Well, they won their election. But whereas the BLM signal decayed after the election was over, COVID is slow to go away. I can’t express how many of my colleagues – highly educated biologists every one of them – remain terrified of catching COVID. They cling to vaccines and masks like a drowning man will cling to any solid object to keep from going under – but in this case, if he just stuck his feet out he’d see that the water’s only a few feet deep. They worry that their healthy children might catch the virus, even though the risk to them is infinitessimal. “Your pandemic is over – their panic continues”, says Peachy Keenan in an article at The American Mind (links from original):
You and I will be fine. We can now abide, even thrive, in the post-pandemic universe, rip off our masks and burn our (fake) vax cards. But what do we do about the mind-flayed women, usually the mothers of young healthy kids, who literally think their children will die without multiple vaccines? Even the WHO admitted that healthy children don’t need boosters. But it’s too late for facts. Hordes of terror-stricken fanatics are already posting photos of their five-year-olds getting their first Pfizer shots on their birthdays, the way you’d post about your 16-year-old getting their driver’s license.
She later posts this quote from a mother who is all too reminiscent of people I encounter every day in my job — according to Keenan, and I whole-heartedly agree, “it’s like reading a dispatch from Mars:”
“I want to scream. The pandemic is not fucking over, because children under 5 cannot get fucking vaccinated. Do not tell me it’s usually really mild for kids. I won’t mention that if I get it, too, I’ll be able to take off the mask I will have been wearing around the clock inside my own home. He’ll get his second and third shots or however many he needs, and eventually he’ll be just like you, as protected as possible, safe enough to go about his toddlery business with COVID being just another risk like accidents or the flu. But we aren’t there yet. And what’s worse than not being there yet is how the world seems to have utterly forgotten we exist.”
So there’s the problem — widespread gaslighting and psychological abuse as a campaign strategy by a party with a vested interest in reducing quality of life for its constituency. In the second part of this essay I’ll consider the long-term effects of this kind of treatment, and how it might be possible to break free from its grip.